
What happens after bariatric surgery? In the first few weeks, most patients receive detailed instructions about healing, hydration and gradually reintroducing food.
Taking your supplements does not always mean your body is absorbing enough.
Here is what to watch for, what should be tested and when treatment that bypasses digestion may be appropriate.
You take your bariatric vitamins. You try to prioritize protein. You may even have bloodwork done occasionally and be told that most things look fine.
But lately, you are more tired than expected. Your hair may be shedding. Exercise feels harder.
You may have brain fog, restless legs, weakness or iron and B12 levels that keep falling despite taking supplements.
It is easy to assume you need a stronger vitamin.
After gastric sleeve, gastric bypass or another bariatric procedure, however, the problem may not be what you are taking. It may be how much your digestive system can absorb.
The short answer: Intravenous IV Therapy bypasses the stomach and intestine. It may help when a clinically important deficiency has been confirmed and oral treatment is not tolerated or does not restore adequate levels.
IV iron is the clearest example after bariatric surgery.
Other deficiencies may be treated more appropriately with oral supplements or injections, depending on the nutrient, the severity and your results.

Click to enlarge
Could poor nutrient absorption be affecting you?
Nutrient deficiencies rarely have one unmistakable symptom. Their effects can overlap with poor sleep, stress, thyroid problems, perimenopause and other health concerns.
Possible signs that deserve a closer look include:
– Persistent fatigue despite adequate sleep
– Reduced stamina or shortness of breath with ordinary activity
– Brain fog or difficulty concentrating
– Hair shedding or brittle nails
– Restless legs
– Headaches, dizziness or feeling faint
– Heart palpitations
– Muscle weakness, cramps or reduced exercise tolerance
– Tingling, numbness or balance changes
– Iron or B12 that remains low despite supplementation
These symptoms do not confirm a deficiency. They are reasons to investigate rather than keep changing supplements based on guesswork.
It is also possible to have depleted iron stores before hemoglobin falls far enough to be labelled anemia. A basic blood count can therefore appear acceptable while ferritin and other iron markers tell a different story.

Click to enlarge
Why might supplements stop being enough?
Bariatric surgery is designed to change how much you can eat and, with some procedures, how food moves through the digestive system. Those changes can improve health, but they can also affect nutrition in several ways:
– Smaller portions can provide less iron, protein, calcium and other nutrients.
– Reduced stomach acid can affect the release and absorption of certain nutrients.
– Food may bypass parts of the intestine where important nutrients are normally absorbed.
– Meat, dairy or other nutrient-dense foods may become difficult to tolerate.
– Nausea or vomiting can reduce food, fluids and supplements even further.
– Acid-reducing medications and metformin may add to certain nutrient concerns.
A supplement can only help if it contains what you need, in an appropriate amount and in a form your body can use.

Click to enlarge
Obesity Canada notes that even some products marketed as post-bariatric vitamins may require additional iron, calcium, vitamin B12 or vitamin D based on laboratory results.
Your type of surgery changes the risk
Procedure | How nutrition may be affected
Gastric sleeve: Smaller food intake and changes in stomach function can contribute to iron, B12, folate, vitamin D or thiamine concerns, even though the intestine is not bypassed.
Roux-en-Y gastric bypass: Smaller intake, reduced exposure to stomach acid and bypassing the upper small intestine can interfere with iron, B12, calcium and other nutrients.
Duodenal switch or biliopancreatic diversion: Greater malabsorption can affect protein, minerals and the fat-soluble vitamins A, D, E and K, requiring close long-term follow-up.
Adjustable gastric band: Malabsorption is less pronounced, but restricted intake, food intolerance or frequent vomiting can still lead to deficiencies.
The risk does not necessarily disappear because surgery happened years ago. Nutrient stores can decline gradually, supplement needs can change and routine surgical follow-up often becomes less frequent with time.

Click to enlarge
Not every deficiency needs an IV
IV treatment solves one particular problem: it bypasses gastrointestinal absorption.
That can be extremely useful when poor absorption or intolerance is preventing an appropriate oral treatment from working.
But the route should be matched to the nutrient and the patient—not selected from a general symptom checklist.
Nutrient or concern | Where treatment may fit
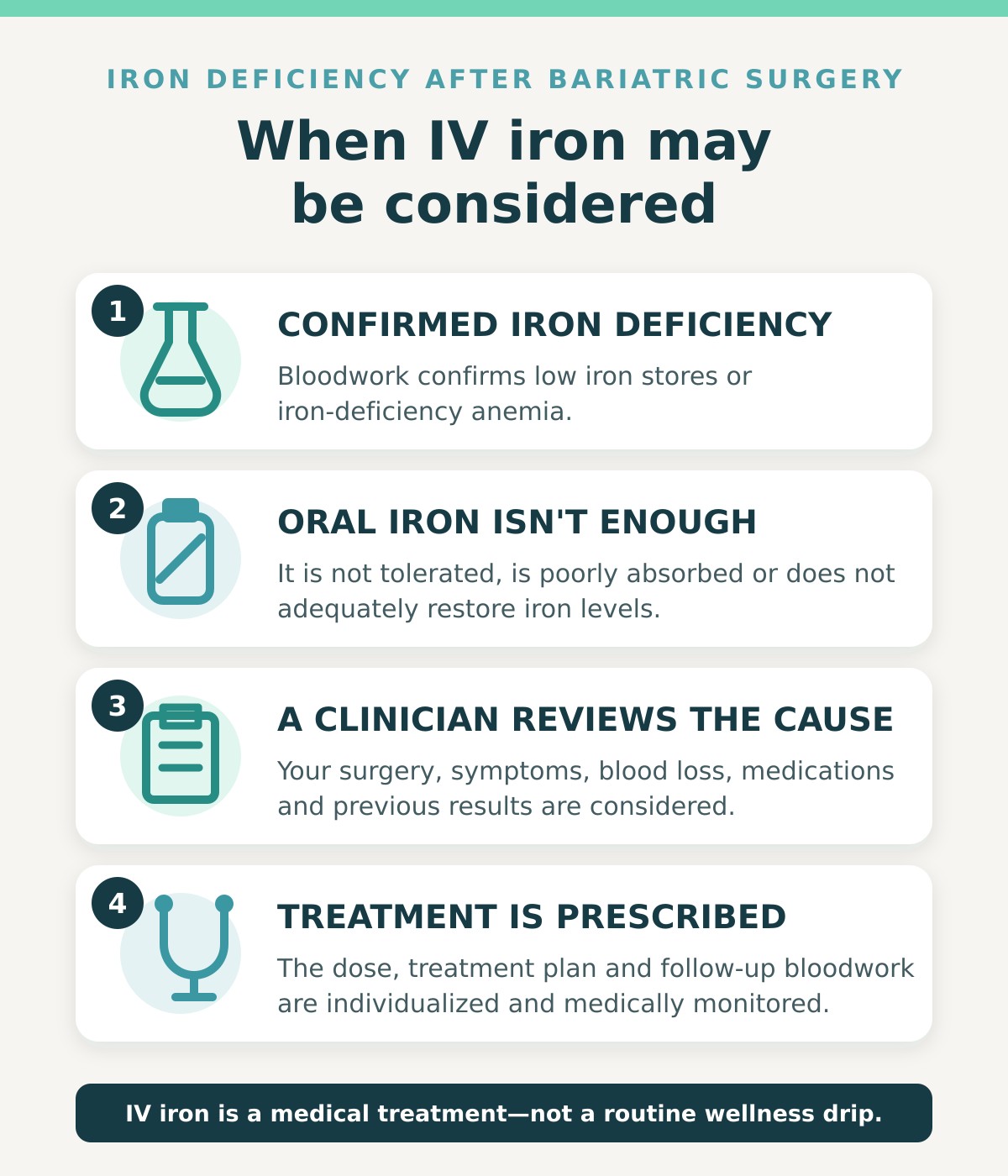
Iron: Oral iron may be appropriate initially. IV iron may be considered when iron deficiency is confirmed and oral treatment is not tolerated, is poorly absorbed or does not restore levels adequately.
Vitamin B12: Depending on the results and clinical situation, B12 may be treated with bariatric-specific oral supplementation, sublingual B12 or injections. An IV is not usually required.
Thiamine (vitamin B1): Prolonged vomiting or severely reduced intake can lead to a serious deficiency requiring prompt medical assessment and, in some cases, urgent intravenous treatment.
Vitamin D and calcium: These are generally managed with carefully selected oral supplementation and follow-up bloodwork rather than routine IV therapy.
Folate, copper, zinc and vitamins A, E and K: Testing and treatment depend on the procedure, symptoms and previous results. High-dose self-treatment can create imbalances and should be avoided.
Dehydration: IV fluids may be used medically, but repeated vomiting or an inability to keep fluids down requires investigation of the cause—not simply a hydration drip.
Why IV iron deserves particular attention
Iron deficiency is a significant long-term concern after bariatric surgery, especially following gastric bypass and in premenopausal women, particularly those with heavy menstrual bleeding.
Smaller portions, reduced stomach acid, difficulty tolerating iron-rich foods and bypassing part of the small intestine can all contribute.
Oral iron can also cause constipation, nausea or abdominal discomfort, and some post-bariatric patients do not absorb enough to rebuild their iron stores.
Clinical bariatric guidelines recommend intravenous iron when confirmed iron deficiency does not respond adequately to oral treatment.
An iron infusion delivers the prescribed dose without relying on gastrointestinal absorption.
It still requires appropriate bloodwork, a medical assessment, an individualized prescription and clinical monitoring.
Click to enlarge
The step many patients are missing: checking whether the plan is working
Symptoms can tell us that something deserves attention. They cannot tell us which nutrient is low, how significant the problem is or whether an IV is the right treatment.
A clinician may consider:
– Complete blood count (CBC)
– Ferritin and iron studies, including transferrin saturation
– Vitamin B12, with additional testing when symptoms and the B12 result do not align
– Folate
– Vitamin D
– Calcium and parathyroid hormone
– Albumin and other markers relevant to protein and overall nutrition
– Electrolytes, kidney and liver markers
– Thiamine, copper, zinc or vitamins A, E and K when the procedure or symptoms indicate
The individual numbers are only part of the assessment. Your clinician should also review which procedure you had, when it occurred, your current supplements and medications, food tolerance, menstrual or other blood loss, digestive symptoms and previous laboratory trends.
Understanding what happens after bariatric surgery long term is important because nutrient stores can decline gradually, even when you take your recommended supplements.
What post-bariatric nutrient assessment looks like at Higher Health
At Higher Health, we do not begin by choosing an IV. We begin by understanding your surgery, symptoms, supplements and bloodwork.
From there, we determine whether oral supplementation, an injection, medically supervised IV treatment or referral back to your bariatric team is the appropriate next step.

Click to enlarge
1. Tell us what has changed
We learn which procedure you had, when you had it, what you are currently taking and what symptoms or laboratory changes you have noticed.
2. Review the right information
We review recent bloodwork when available and determine whether additional testing may be helpful. We look at the pattern rather than relying on one isolated number.
3. Match treatment to the findings
Your plan is based on what the assessment shows. If IV iron or another treatment is medically appropriate, we explain why, what is involved and how the response will be monitored.

Click to enlarge
Taking your supplements but still not feeling right?
You should not have to keep changing products and hoping something works.
Book a complimentary 15-minute call with Higher Health Naturopathic Centre & IV Lounge in Toronto.
Tell us which bariatric procedure you had, what symptoms you are experiencing and whether you have recent bloodwork.
We will help you determine whether a nutrient assessment or targeted treatment may be an appropriate next step.
Book Your Complimentary 15-Minute Call
If you have persistent vomiting, cannot keep fluids down, have severe abdominal pain, black or bloody stools, fainting, chest pain, significant shortness of breath or new confusion, weakness, numbness or balance problems, seek urgent medical care rather than waiting for a routine appointment.
Frequently Asked Questions
Can nutrient deficiencies appear years after bariatric surgery?
Yes. Nutrient stores can decline gradually, food tolerance and medications can change, and supplement needs may be different several years after surgery. Long-term monitoring remains important even when you initially felt well.
Can gastric sleeve affect iron and B12?
Yes. Gastric sleeve does not bypass the intestine, but smaller food intake and changes in stomach function can still contribute to iron, B12 and other nutrient concerns.
Does every bariatric patient need IV therapy?
No. Many deficiencies can be managed with appropriate oral supplementation or injections.
IV treatment is most useful when there is a specific clinical reason to bypass the digestive system. IV iron is a well-established example when oral iron is not tolerated or does not adequately correct confirmed iron deficiency.
Should I stop my bariatric vitamins before being tested?
Do not stop prescribed or recommended supplements unless your treating clinician advises you to do so. Bring a complete list—or photographs of the labels—to your appointment so the ingredients and doses can be reviewed.
Can Higher Health work with my bariatric or primary-care team?
Post-bariatric care may involve several healthcare professionals.
When appropriate and with your consent, findings and treatment recommendations can be coordinated with the clinicians involved in your care.
*This article is for educational purposes and is not a substitute for individualized medical care. Continue the supplements and follow-up recommended by your bariatric surgical team unless your treating clinician advises otherwise.
References:
Obesity Canada: Bariatric Surgery—Post-Operative Management
https://obesitycanada.ca/wp-content/uploads/2025/03/14-Canadian-Adult-Obesity-CPG-Bariatric-Surgery-PostOperativeMgmt.pdf
American Society for Metabolic and Bariatric Surgery: Integrated Health Nutritional Guidelines
https://asmbs.org/wp-content/uploads/2017/06/ASMBS-Nutritional-Guidelines-2016-Update.pdf
American Society for Metabolic and Bariatric Surgery: Life After Bariatric Surgery
https://asmbs.org/patients/life-after-bariatric-surgery/
Obesity Canada: Canadian Adult Obesity Clinical Practice Guidelines
https://obesitycanada.ca/healthcare-professionals/adult-clinical-practice-guideline
The Protein Number You’ve Trusted for 70 Years Was Never Meant to Keep You Strong
Is IV Therapy Safe? Why We Assess (and Sometimes Decline) Before Any Drip
GLP-1s and Perimenopause
